Enter your email address
Submit

![]()
![]()
![]()


 , Afsaneh Riazat2 , Sheari Sury2 , Negar Saffarinia2 , Zahra Damerchi2 , Mostafa Pouyakian *3
, Afsaneh Riazat2 , Sheari Sury2 , Negar Saffarinia2 , Zahra Damerchi2 , Mostafa Pouyakian *3
✅ From among the four simulated scenarios, the fourth one, which is the increase in staff welfare parameters, had the most impact on reducing the burnout of Ardabil Regional Water Company employees.
P atient safety is a key component of quality of care [1, 2] and a major concern of any health care system [3-5]. Error is also an integral part of human life [6]. These two factors have irreparable consequences in some sensitive occupations such as medicine and nursing that are related to the patient's life.
From a financial standpoint, more than $ 17 billion is spent annually on medical errors in the United States. Error rates in health systems around the world are high, affecting one in 10 patients. In addition, approximately 7% of these errors are fatal [10]. In Iran, medical errors and convictions of 51% of nurses in court cases confirm the importance of these errors [11].
Lewis et al. see nurses' involvement in mistakes as a vague problem that needs to be explained. They also state that medical errors occur when medical care providers, such as nurses, make the wrong decision or use the wrong method [8]. The law defines nursing error as non-compliance with diagnostic, treatment, and care standards. In the legal literature, the error is also classified as negligence or violation of laws [13]. However, Sanago et al. consider nursing errors to be an action that endangers the patient's life or causes harm to the patient [14].
In a review study, Madadi and Jaafaripooyan compared nurses' medication errors and provided solutions to prevent errors in Iran and developing countries. The main causes of medication errors in Iran were the shortage of nurses and staff in selected industrial countries. They also considered the role of education in providing joint solutions in Iran and developing countries more important. On the other hand, the implementation of error reporting systems, the use of electronic prescriptions, consultations of clinical pharmacists, and the existence of pharmacology books in the sections of the solutions are presented in this study to prevent drug errors [15].
In a systematic review study conducted by Keers et al. in the period 1985-19000 with the aim of investigating drug management errors, the three most common errors were the wrong dose of the drug at the time of administration, the wrong time of drug administration, and forgetting to prescribe medication to patients [17]. In a systematic review by Kiekkas et al., six studies over a period of time (1985-2008) aimed to detect nurses' medication errors through direct observation. Wrong dose and inappropriate time of drug administration, as well as the omission of some dose of the drug, are among the most common errors identified in this study. Also, based on the results of this study, the diagnosis of factors affecting drug errors is inconclusive and continuous monitoring is one of the cases to reduce drug errors [18]. In their study, Flynn et al. found that direct observation and recording of nurses 'errors by a trained nurse was far more reliable and accurate than identifying nurses' errors through chart analysis (by researchers) and self-reporting [19].
Looking at the previous studies, it is clear that in the studies, more attention has been paid to the solutions for nurses' medication errors. Also, less research has been done to identify and present nurses 'errors that are caused by managerial or environmental factors, and a study should be conducted on collecting nurses' errors, their reasons, and solutions in the last 10 years. However, in addition to classifying nurses 'errors, this article provides a comprehensive overview of the causes of nurses' errors and appropriate strategies to prevent their occurrence from the studies of the past 10 years in this article; therefore, according to what has been said in this study, we have examined the types of errors of nurses and its causes, strategies to reduce errors, causes of non-reporting errors and strategies to improve it. Due to the dispersion of studies, this study has summarized them for comprehensive coverage of the mentioned topics.
The present study is a review-narrative study. The statistical population of the present study includes all studies related to nurses 'errors in terms of performance, review, retrieval, communication, and selection, how to collect errors, causes, and strategies to reduce nurses' errors that are published and accessible. Inclusion criteria are all articles published in English and Persian from 2008-2018 on the types of nurses' errors, how to collect information, causes, and related reduction strategies.
Three internal databases including SID, Magiran, and Iran Medex with Persian keywords “human error” and “nursing error” and English words “Nursing Error’’ and “Nursing human error” have been searched in five external databases including Google Scholar, PubMed, Scopus, Science Direct and Springer. The selected keywords were due to more focus on nurses' errors and their proper classification, as well as due to consistency with the purpose of the present study. Initially, 8864 articles were found, which due to the multiplicity, was limited to the period of 2008-2018, and as a result, it was reduced to 1568 articles. In the next step, 574 articles that were open access and full text were selected; the reason for choosing open access and full-text articles was the importance of the details mentioned in the text of the articles. Also, 374 articles were deleted due to irrelevance (medical error, laboratory examination, legal issues of error, medical ethics, and midwifery error examination). According to their titles and abstracts, 90 articles were reviewed due to repetition, nursing error modeling, and a case study related to an accident, leaving a total of 49 articles for the present study. Figure 1 shows the complete article selection process.
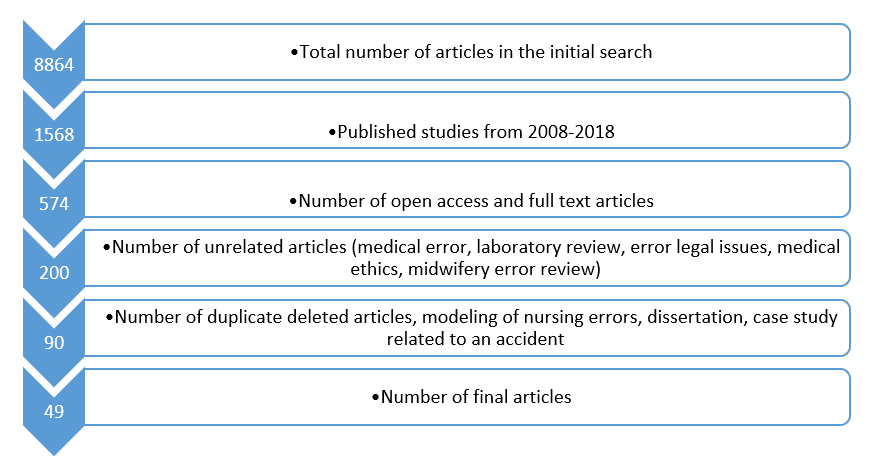
Figure 1. How the articles were selected from databases
Different divisions can be considered for nurses' errors. Nurses' mistakes can be divided into hidden and active categories. Active errors include whether or not nurses act, whose activities can have adverse effects, and hidden errors include errors that are beyond the direct control of nurses and result from incorrect management decisions and structural weakness in organizations [14]. Nurses' errors can also be divided into human, technological or systemic errors [8]. In the SHERPA method, we can refer to various types of functional, retrieval, visit, communication, and selective errors. In this method, during the whole process of job task analysis, major external errors, and errors with psychological mechanisms can be identified. In this study, the types of errors have been studied based on the classification of the SHERPA method.
Table 1 lists the final studies selected based on the names of the authors of the articles, the year, and the method of data collection. The Table also shows that the authors of selected articles in the past 10 years have studied in which areas of nurses' errors, the cause of their errors, identifying barriers to reporting errors and strategies to reduce errors [20-70]. Table 2 also shows the list of internal and external studies based on the applied method and technique and the number of articles reviewed by the mentioned method or techniques.
Table 1. List of studies by author, year, data collection method and main context of studies based on identification, causes, reporting barriers and error reduction strategies
| Error reduction strategies | Barriers to reporting errors | Investigate the causes of the error | Error detection | Data collection method | Year | Author | Row |
| * | questionnaire | 2018 | Shali et al. | 1 | |||
| * | questionnaire | 2018 | Sharbaafchi zadeh et al. | 2 | |||
| * | questionnaire | 2018 | Azarabad et al. | 3 | |||
| * | SHERPA | 2018 | Ghiyasi et al. | 4 | |||
| * | questionnaire | 2018 | Chen et al. | 5 | |||
| * | questionnaire | 2018 | Kohan et al. | 6 | |||
| * | * | * | FMEA | 2017 | Askari et al. | 7 | |
| * | * | TRACer | 2017 | Babaei pouya et al. | 8 | ||
| * | * | SHERPA | 2017 | Mirzae Aliabadi et al. | 9 | ||
| * | Checklist | 2017 | Foo et al. | 10 | |||
| * | Checklist and questionnaire | 2017 | Alemu et al. | 11 | |||
| * | * | * | Checklist and questionnaire | 2017 | Fathi et al. | 12 | |
| * | * | interview | 2017 | Ajri Khameslou et al. | 13 | ||
| * | * | * | * | questionnaire | 2016 | Ebrahimipour et al. | 14 |
| * | * | questionnaire | 2016 | Ghorbanpour Diz et al. | 15 | ||
| * | interview | 2016 | Peyrovi et al. | 16 | |||
| * | * | * | NPSA | 2016 | Adibi et al. | 17 | |
| * | * | * | questionnaire | 2016 | Winsett et al. | 18 | |
| * | * | questionnaire | 2016 | Zeighami et al. | 19 | ||
| * | - | 2016 | Bravo et al. | 20 | |||
| * | interview | 2016 | Samsiah et al. | 21 | |||
| * | questionnaire | 2016 | Weaver et al. | 22 | |||
| * | - | 2016 | Morelock et al. | 23 | |||
| * | * | questionnaire | 2016 | Shahabi et al. | 24 | ||
| * | * | questionnaire | 2016 | Saki et al. | 25 | ||
| * | questionnaire | 2016 | Rahimi et al. | 26 | |||
| * | * | * | Event review | 2015 | Wan et al. | 27 | |
| * | * | SPR-H | 2015 | Mohammadfam et al. | 28 | ||
| * | * | Survey | 2015 | Roth et al. | 29 | ||
| * | Checklist and questionnaire | 2015 | Feleke et al. | 30 | |||
| * | questionnaire | 2015 | Nwozichi et al. | 31 | |||
| Checklist | 2015 | Bozorgzad et al. | 32 | ||||
| * | questionnaire | 2015 | Nouhi et al. | 33 | |||
| * | holding a committee | 2015 | Wu et al. | 34 | |||
| questionnaire | 2015 | ahangarzade rezaie et al. | 35 | ||||
| * | * | * | CREAM | 2014 | Mohammadfam et al. | 36 | |
| * | questionnaire | 2014 | Hesari et al. | 37 | |||
| * | questionnaire | 2014 | Zhu et al. | 38 | |||
| * | questionnaire | 2014 | Nouhi et al. | 39 | |||
| questionnaire | 2013 | Pazokian et al. | 40 | ||||
| * | * | questionnaire | 2013 | Habermann et al. | 41 | ||
| * | * | * | questionnaire | 2013 | Rahimian Boogar et al. | 42 | |
| SHERPA | 2013 | Kermani et al. | 43 | ||||
| * | * | questionnaire | 2013 | Mirzaei et al. | 44 | ||
| * | * | * | questionnaire | 2012 | Bagaei et al. | 45 | |
| * | questionnaire | 2012 | Salavati et al. | 46 | |||
| * | * | interview | 2011 | Wilkinson et al. | 47 | ||
| * | * | questionnaire | 2010 | Eslamian et al. | 48 | ||
| * | * | - | 2009 | Green et al. | 49 |
Table 2. List of Iranian and foreign studies based on the method and technique used and their frequency
| Studies | Data collection method | Number of articles |
| Studies in Iran country (31) | questionnaire | 15 |
| interview | 2 | |
| SHERPA | 3 | |
| Checklist and questionnaire | 1 | |
| Checklist | 1 | |
| Cream | 1 | |
| FMEA | 1 | |
| Tracer | 1 | |
| NPSA | 1 | |
| SPRH | 1 | |
| Study abroad (18) | questionnaire | 11 |
| interview | 2 | |
| Checklist and questionnaire | 2 | |
| Checklist | 1 | |
| Event review | 1 | |
| Holding committee | 1 | |
| Survey | 1 |
According to Table 2, in 15 studies out of 31 domestic studies and 11 studies in foreign studies, nurses' errors were examined by a questionnaire. Also, different methods have been used to identify nurses' errors in domestic studies as opposed to foreign studies. In the present study, nurses' errors were divided into five categories based on SHERPA method: functional, review, communication, retrieval and selective errors. Based on the rate mentioned in various studies, nurses' errors can be classified into functional errors [23, 33, 34, 39, 40, 52, 53, 59, 62, 64, 69], review [32], communication [23], retrieval [53, 63] and finally selectively [34, 53, 63, 64]. Table 3 also shows the division of the errors mentioned in the selected articles into functional, review, communication, retrieval and selective errors. Figure 2 also shows the number of errors obtained and classified using the SHERPA method from the review of various articles.
Table 3. Classification of errors mentioned in the articles into functional, review, retrieval, communication and selective errors according to SHERPA method
| Functional errors | Failure to collect and review the patient's medical history, lack of review of laboratory tests, evaluation, action and control of the patient in the wrong direction, delayed care, recording incomplete and incorrect patient information in the file, additional and unnecessary action, setting too much or too little device, sitting Hands, not using masks and glasses while working [58], placing the thermometer in less than necessary time in the relevant place [38], error in giving the medicine [22, 66, 67], error of the drug administration (managing the time and dose of the drug) [32], technical errors such as incorrect cardiopulmonary resuscitation measures [33], wrong timing error [22, 51, 64, 67, 69], wrong path error [33,52], drug injection and injection rate [22], identification of the patient [66], Violation of regulations [39], not to observe the sterile technique, Reaction to foreign body remaining at the surgical site, Reaction to blood and blood products [70], Respiratory care [62], Injection of wrong Drug, error in reading the expiration date of the drug [34], forgetting to give the drug to the patient [37,38] |
| Review errors | Checking incorrectly for the expiration date of the medicine, giving the illicit medicine, ignoring the side effects of the medicine, not monitoring the patient's condition, not monitoring during and after the blood transfusion, error in hearing or visual diagnosis of device alarm and vital signs of the baby, forgetting to perform the operation, forgetting instructional information, mistake in remembering the technique of performing the action, making late or weak decisions, not having a work plan, error in performing the action [31] |
| Recovery errors | Immediate action for dysrhythmia, failure of initial resuscitation, code announcement, and initiation of cardiopulmonary resuscitation, incorrect code declaration [52] |
| Communication errors | Unreadability of the doctor's prescription, early or late interventions, the relationship between the doctor and the nurse, error in writing the patient's report after each examination [22], use of medication acronyms [63] |
| Selected errors | Error in the dose of the drug [33, 52, 63], error in reading the name of the drug [33] error in choosing the drug, error in prescribing (giving) the drug [31] |
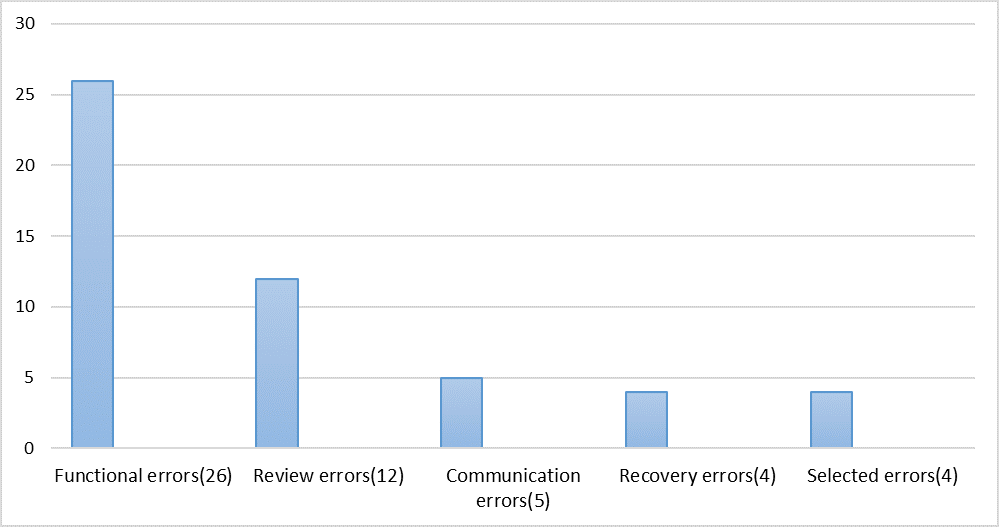
Figure 2. Errors classified by SHERPA method from review of various articles
Ajri-Khameslou et al. have investigated the factors affecting nurses' error in the intensive care unit [42]. Regarding the causes of error, we can point to four main categories: factors causing error related to the nurse [4, 24, 25, 26, 30, 31, 37, 39, 43, 44, 51], factors causing errors related to the organization [22, 23, 25, 29, 37, 43, 44, 49], factors related to intensive care and ward [23,29,33,41, 43, 48, 49] and factors related to the patient [29, 42]. The four main categories of error-causing agents and their subclasses are presented in Table 4.
| section | subsection |
| Nursing-related error factors | Nurse education and skills [24, 26, 38] Lack of knowledge [23, 36, 38, 70], Fatigue [42, 43, 48, 68], Neglect, Routine disruption, Negligence during care [42], Nurse to physician Notification in a timely manner [43], problems recording nursing report [43], fear of reporting, nurse injured by the object, communication problem [25, 29], lack of critical thinking [29], nurse activity outside work, fast work Problems with policies and guidelines, Nurse placement in unfamiliar situations [29], Fatigue due to lack of sleep [29, 43], Familiarity with medications, Nurses' mental and physical problems, Not taking duty seriously, Responsibilities outside of job description, Excessive attention, Forgetfulness and carelessness, risky and reckless behaviors, drug use [31, 50], distraction [70] |
| Factors causing errors related to the organization | Management and coordination aspects of the group [36], Inadequate communication between the manager and employees, Lack of supervision, Organizational policies, Work culture, Defective equipment [24, 42], Lack of in-service training and punitive atmosphere, Physical conditions [28], Heavy workload and shift work [22, 36, 43, 68, 70], use of unprecedented manpower, lack of nursing staff and insufficient assistants and staff [42], lack of comprehensive instructions [22], inadequate training, lack of appropriate training facilities in the workplace [ 21], the indifference of managers to education, the reproachful attitude of managers and colleagues, high acceptance and discharge, unavailability of drugs, damaged and inappropriate label of drugs [48] |
| Error factors related to intensive care | Crowded and busy environment [40, 42, 48], irregular and unpredictable care, difficulties in identifying patients due to their short stay in the emergency department [28, 42], early or late medication interventions [22], inconsistencies in team communication and teamwork [25, 32, 42], environmental conditions [25, 28, 32], doctor's orders by phone, illegible medical orders, lack of proper facilities and equipment and device failure [47] |
| Factors causing the patient-related error | Patient’s critical conditions, different language of patients, patient’s companion’s intervention in treatment [29, 42] |
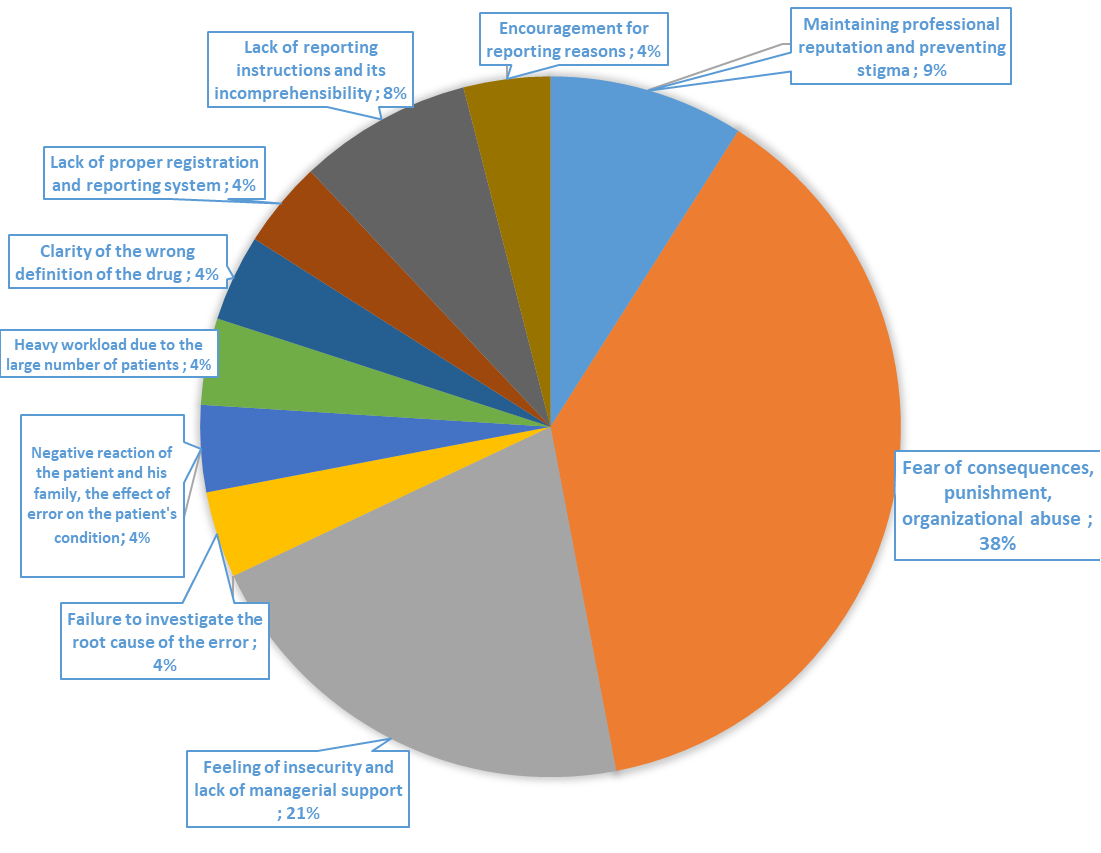
The major barriers for reporting nurses' errors identified in the studies are as follows:
A) Maintaining professional reputation and preventing stigma [23, 65]
B) Fear of consequences, punishment, organizational abuse [22, 23, 41, 44, 48, 63, 65, 70]
C) Feeling of insecurity and lack of managerial support [22, 23, 32, 68, 70]
D) Failure to investigate the root cause of the error [23]
E) Negative reaction of the patient and his family, the effect of error on the patient's condition [32]
F) Heavy workload due to the large number of patients [23]
G) Clarity of the wrong definition of the drug [48]
H) Lack of proper registration and reporting system [23]
I) Lack of reporting instructions and its incomprehensibility [44, 51]
J) Encouragement for reporting reasons [31].
Figure 3 also shows the percentage of major barriers to reporting nurses' errors in various articles.
In general, the nurses' error reduction strategies that have been presented in the articles include the following:
A) Development of standard strategies and guidelines for nurses [30, 36]
B) Nursing education [20, 23, 33, 46, 50]
C) Preparing a list of types and causes of most nursing errors and delivering it to nurses [56]
D) Establishment of error reporting and recording system [44]
E) Management controls [22, 25, 32, 33, 36, 44, 46, 50,59]
F) Creating a culture of learning from error and preventing it instead of a culture of punishment and improving the culture of the workplace [56]
G) Allocating adequate and healthy equipment in the hospital [27]
H) Use of systems to ensure the correct transfer of information and development of patient transfer protocols [58]
I) Application of all main systems and rules of clinical nursing [58].
The aim of this study was to investigate the types and causes of errors of nurses, the reasons for not reporting them, and strategies to reduce errors in various studies. Reviewing different studies showed that in the period of 2008-2018 (Table 1), domestic studies compared to foreign studies have identified more types of errors, their causes, and barriers to reporting nurses' errors and have provided more solutions. In studies conducted in Iran, researchers have been more effective in investigating the causes of error and less in examining the reasons for barriers to reporting errors by nurses [24, 60]. In foreign studies, the reasons for not reporting and the types of errors have been studied almost equally, and most of the studies have been in the field of investigating the causes of errors [20, 31, 33, 41]. Also, in selected articles of Iranian and foreign authors based on Table 2, mostly questionnaires and checklists have been used. In general, in future studies in the country and abroad, more research can be done on the reasons for not reporting nurses, and even the effect of practical interventions for reporting nurses 'errors, such as designing studies for creating a culture of reporting errors and examining the effect of nurses' training on reporting nursing errors.
Based on the findings of the present study (Figure 2), the most identified nursing errors were functional errors of nurses with 26 cases; in other words, functional errors in the nursing system meant ineffective health action at the appropriate time and place. Among these, the multiplicity of functional tasks due to the nature of the nursing profession can be one of the reasons for this problem [58]. Also, the lowest number of errors was related to retrieval and selection errors with 4 cases. In the event of an error, a single factor can rarely be identified, but according to Table 4, a set of factors causes an error to occur [42]. Therefore, in order to prevent them, one should pay attention to a set of solutions provided in the health management system. In the study of Zeighami et al., which examined the causes of nurses' errors, according to nurses, the highest and lowest causes of nursing errors were related to the management and coordination of the team, respectively. Also, in relation to the management aspect, the most common and least important causes identified by nurses are: "Inadequate organization of nursing staff in the unit" and "Lack of proper management policy and guidelines", respectively. Regarding nurses' training and skills, the most common and least common causes reported by nurses are "not using trained and specialized nurses" and "insufficient familiarity with the method of using equipment", respectively. Also, in relation to physical and environmental conditions, the most common and least important causes identified by nurses were "inappropriate behavior of patients and their relatives" and "long distance between the nursing station and the patient's room or bed", respectively. On the other hand, in relation to team coordination, the highest and lowest causes by nurses are "inappropriate relationships between nursing team members" and "inappropriate behavior of supervisory team members when diagnosing nursing errors" [36]. Mentioning these points in various studies and being aware of them causes proper management which will lead to reducing the causes of nurses' errors in health and care settings.
Of the studies cited, 38% pointed at "fear of consequences, punishment, organizational misconduct" and 9% of them at "maintaining the professional reputation and preventing stigma" as the reason for non-reporting of errors by nurses, and cases of "encouraging reporting", "lack of registration system" and "correct reporting", "unclear definition of medication error", "heavy workload due to a large number of patients", "negative reaction of the patients and their family", "the effect of the error on the patient's condition" and "not investigating the main cause of the error" (4 Percentage) have been reported in various studies as a reason for non-reporting of nurses.
Hospital and ward managers play an important role in preventing nurses from making mistakes. They are usually responsible for using the protocols and instructions provided to prevent nurses from making mistakes [36]. The first step in reducing nursing errors in hospitals is management controls. As mentioned in Wan's study [21], since according to the results of several studies, factors such as shortage of nursing staff, heavy workload, and inadequate distribution of nurses in different wards of the hospital are important factors affect the incidence of nursing errors, accuracy in providing management solutions can play an effective role in reducing errors. Proper distribution of nursing staff and increasing their number [22], providing hours for their comfortable sleep, creating a dynamic environment and a system for honest reporting of errors and the reasons for their occurrence by nurses [36], use of specialized nursing workforce [32], increasing the motivation, empathy and proper interaction of managers with nursing staff, discussion sessions between managers and nurses, the positive response of managers to error reporting [48], the non-disciplinary approach of managers to error [44 ], monitoring careful supervision and frequent review, more supervision of hospital managers especially in unconventional work shifts, careful scheduling [46], and improving the environmental conditions of the wards such as reducing noise and improving lighting design [33] are some of the solutions found in the literature.
Other strategies suggested by Pazokian et al. were to reduce errors including training courses [27] that include points like the importance of identifying and reporting medication errors, training for early entry staff, conducting error analysis training courses, and ongoing patient safety training. It also reduces errors with medication information retraining classes. Other ways to reduce errors include creating cultures of error reporting and error learning [36], providing adequate equipment for the hospital, strengthening teamwork [22, 25, 33], basic familiarity with the native languages of the country, identifying the population with special vulnerabilities for nursing errors such as older patients, correcting the methods of recording the nursing report [36], computerization of medical instructions and the treatment process of patients [58]. Limitations of the study on nurses' errors in the studied studies included the reluctance of employees to complete the questionnaires, their reluctance to be seen by the reader at work, not having access to all nurses due to shifts, not participating in the self-reporting process [29,34] which it seems that more detailed attention can be paid to them in future studies. It is also recommended that researchers identify errors that may occur as intentional errors in future studies; for example, while a nurse may know that implanting a venous line for a patient with dementia requires an informed consent signed by their companion, he or she may do so with the patient's consent given the importance of medication schedules. In this case, a deliberate and benevolent error occurs without the intention of harming the patient. Also, in examining nursing errors, the situations in which nursing errors occur should be considered. The cause of the error, environmental factors, behavioral theories, prevailing perceptions, human error prediction, and ethical
The benefits of the view of articles lead to the provision of appropriate services in medical centers, proper planning for hospitals by managers, the improvement of nursing education in universities, as well as increasing the awareness of nurses and their officials in the health services. However, in studies, new methods of risk identification have been less used. The authors also pay less attention to past studies to identify the causes of errors; because in many studies reviewed in this paper, similar causes have been found in several studies. Researchers should also examine barriers to reporting nurses 'errors, designing practical interventions to reduce nurses' errors, or examining the errors that nurses have intentionally committed.
Nursing errors have been studied in different ways. These studies are not only to identify nurses' errors but also with the aim of strengthening the acknowledgment and awareness about possible causes and preventing factors. The benefits of this view of articles lead to the provision of appropriate services to medical centers, proper planning for hospitals by managers, and the advancement of nurses' training.
The authors are grateful to all those who assisted in the writing of this article.
The authors declared no conflict of interest.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |