Enter your email address
Submit

![]()
![]()
![]()
✅ Given the correlation between the ROSA results and the CMDQ, they can be used together. The change should be considered immediately for persons who are in intervention group.
Few jobs can be found today that do not use computers. Advances in technology have not only reduced musculoskeletal disorders (MSDs) but also increased them due to ergonomics (1). More than 60% of office workers in developing countries complain from physical discomfort, many of which are related to MSDs. Its prevalence is reported to be 15% -70% due to the type of work and contact time between the workstation and the computer station (2,3), which is the result of poor ergonomic design (5). In 2013, the World Health Organization (WHO) classified MSDs as the second prevalent job related disease (6). Depending on computer work, these disorders occur in the first stage in the upper extremities (7). Low back disorders are also common depending on the state and time of sitting (8). As improper posture at work is one of the most important risk factors for MSDs, in many risk assessment methods for MSDs, posture analysis is considered as the focus and basis of evaluation (9). Due to the fact that bank employees do a lot of their work with computers and their body position and equipment may lead to MSDs, this study was conducted to determine the prevalence of musculoskeletal disorders in Melli Bank employees and its relationship with administrative stress.
This cross-sectional descriptive study was conducted as a census on the employees of the Melli Banks of North Khorasan Province (with 25 branches, each with an average of 8 employees). People who worked with computers and had at least 1 year of experience entered the study. Finally, 173 people were examined. First, the job was reviewed and the demographic information of the individuals was recorded. The Cornell Musculoskeletal Disorder (CMDQ) questionnaire (with a validity of 0.960-0.828 and a reliability of 0.986) (10) was then given to people after justification to record the frequency of their discomfort / pain from body parts and its impact on work capacity during the last week (11). Each person who received a CMDQ was also tested for risk factors for the person's work-related disorders. Individuals were also analyzed regarding their posture by ROSA method (with internal and intermediate reliability of observers 0.88 and 0.91, respectively). Risk factors were analyzed according to the ROSA checklist and the final score was categorized into three categories (7). Finally, the data was entered into SPSS 20 (SPSS Inc., Chicago, IL., USA) to estimate the prevalence and risk factors for disorders. The prevalence and risk factors were reported by descriptive statistics. The relationship between the prevalence of distress and the risk of their causative factors, demographic layout and specifications was assessed by Spearman correlation test and significant level (P<0.05).
The results of posture analysis by ROSA method are categorized as frequency and percentage in Table 2. The average ROSA score was 4.73±0.793 between 3 and 9.
The results of the prevalence of musculoskeletal disorders by the CMDQ technique showed that the mean scores were 181.004±103.63 and between 1650-2. The results of correlation by Spearman test showed that there is a significant relationship between ROSA and CMDQ results (P=0.021, R=0.175). CMDQ showed that there was a significant relationship between age and work experience with the prevalence of musculoskeletal disorders (P=0.037, R=0.159). Also, Kruskal–Wallis test showed a significant relationship between education level and CMDQ results (P=0.38). In other demographic characteristics, this relationship was not significant. Examination of the discomfort of the limbs showed the highest prevalence of neck discomfort followed by the lower back, upper back, right shoulder and then other areas. Table 1 shows the prevalence of various organs. Figure 1 also shows the percentage of prevalence and severity of reported discomfort in these areas. The ROSA chair section score was statistically correlated with the final CMDQ score (P=0.021).
Table 1. Demographic characteristics of individuals
| M | SD | Minimum | Maximum | |
| Age | 44.80 | 6.587 | 28 | 68 |
| Work history | 15.66 | 5.866 | 1 | 28 |
| BMI | 25.4680 | 3.12819 | 19.32 | 38.63 |
| Number of samples | 173 | |||
Table 2. Frequency and classification of the final score of the ROSA method
| class ROSA | Region | Frequency | % |
| 3< | Safe | 0 | 0 |
| 3-5 | Alert | 63 | 36.4 |
| +5 | Intervention needed | 110 | 63.6 |
| Total | 173 | 100 | |
Table 3: Percentage of prevalence of discomfort in different areas of the body
| اBody organs | % | Body organs | % | |
| Neck | 53.8 | Right wrist | 33.5 | |
| Lower back | 49.7 | Left wrist | 32.9 | |
| Upper back | 48 | Right thigh | 32.9 | |
| Right shoulder | 47.4 | Left thigh | 30.6 | |
| The residence | 44.5 | Right knee | 39.9 | |
| Left shoulder | 41 | Left knee | 43.9 | |
| Right arm | 34.1 | Right leg | 38.7 | |
| Left arm | 31.2 | Left leg | 34.7 | |
| Right forearm | 37.6 | The sole of the right foot | 30.1 | |
| Left forearm | 34.1 | Left foot | 35.3 | |
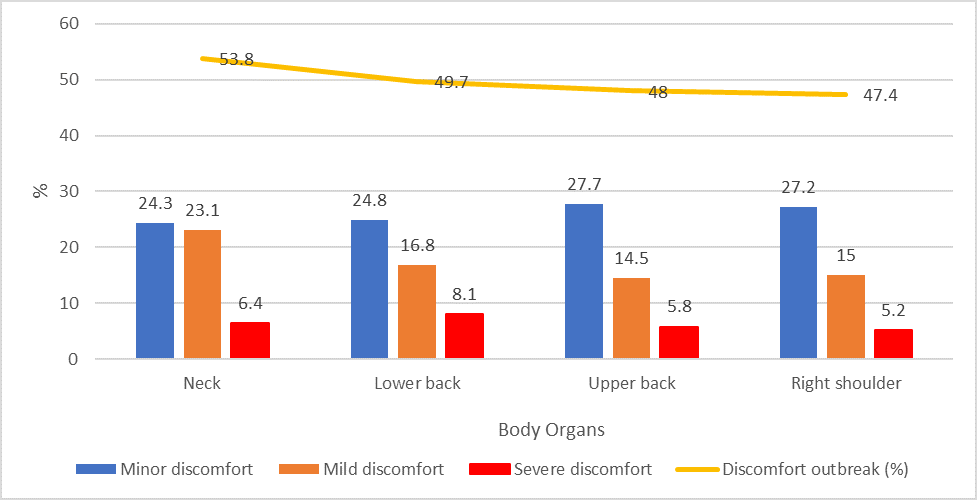
Figure 1. Percentage of outbreaks of discomfort in the limbs and its severity
The average ROSA score was 0.793±4.73. Of postures, 63.6% were part of the intervention level that needed further evaluation and changes had to be made immediately. The study of Sohrabi et al. On 71 administrative staff of Isfahan University of the Arts, which was estimated at an average of 1.9±4.89 (14) and other studies (8,9,12,13) considering the ROSA score, is consistent with the present study. Aneela Umar et al.'s study of 100 employees at Melli Bank Faisal Abad found that the average ROSA score was 0.98±6.74 and the score of 90% of the participants was more than 5, which is higher than the present study. The correlation of ROSA and CMDQ results is consistent with the study of Sohrabi et al. (14), Frost et al. (8) and Sonne et al. (7). But it is inconsistent with Akbari et al.'s study that the reason could be the low risk of developing MSDs. Of the 276 people, only 10 were at risk (17). The significant relationship between work experience and prevalence of MSDs is consistent with the studies of Samaei et al. (12), Gerr et al. (18), Ghanbari et al. (9), and Choobineh et al. (19). The significant relationship between level of education and MSDs is consistent with the study of Frost et al. (8) and non-aligned with the study of Choobineh et al., which could be due to the dispersion of participants' education level (19). The highest degree of discomfort was related to the neck and then the back which was in accordance with the study by Janwantanakul et al., that studied 1,185 administrative staff members, and reported the most discomfort in the neck, lower back, and other areas (24); it was also in line with other studies (12,15,20,21,23,25). The ROSA chair section score was associated with the final CMDQ score, which indicated that the chair plays an important role in preventing MSDs. In this study, chairs and monitors played a more important role. Although there was no significant relationship between the monitor and the neck, this can be due to reasons such as: the score of the monitor section in addition to the neck posture is affected by things like light, etc. and the static state of the neck is not evaluated. In CMDQ details, there was a significant relationship between the neck and upper back (P=0.03), as well as between the neck and shoulders (P=0). This has been confirmed in the study by Szeto et al. (29).
A large part of the postures were placed in the area of the need for intervention. The interventions should be done faster. There was a good correlation between the results of ROSA and CMDQ, which shows that musculoskeletal disorders are related to people's jobs and can be used together to assess and determine the prevalence of musculoskeletal disorders. The most common disorders were in the neck and lower back, which were related to working conditions and equipment such as monitors and chairs. Modifications should be made to the ergonomic seat and equipment layout, such as the monitor. Of course, it is better to visit each station separately. In addition to engineering interventions, teaching ergonomic principles can play a significant role in reducing disorders. One of the limitations of the study was the higher number of men (more than 97%), which led to inability of an assessment regarding gender.
The authors thank all those who helped them writing this article.
The authors declared no conflict of interest.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |